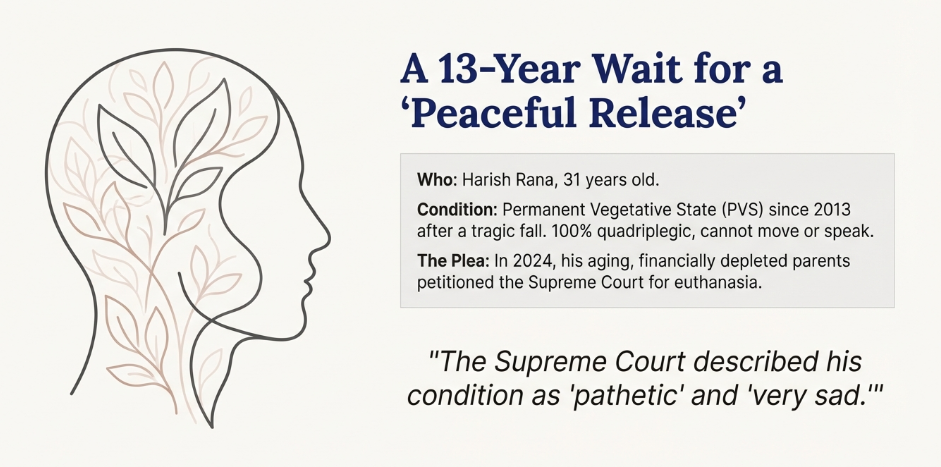
The Harish Rana case involves a 31-year-old man in a Permanent Vegetative State (PVS) for over 13 years following a tragic fall. In 2024, the Supreme Court initially refused his parents’ plea for euthanasia, ruling that removing a feeding tube constitutes “active killing” rather than passive withdrawal of life support.
Recently, the Court began revisiting the case to determine if clinically assisted nutrition—like Harish’s gastrostomy tube—should be legally reclassified as “life-sustaining medical treatment.” With recent medical reports describing his condition as “pathetic,” the Court has scheduled a rare personal meeting with his parents for January 13, 2026, to decide on a “peaceful release.”
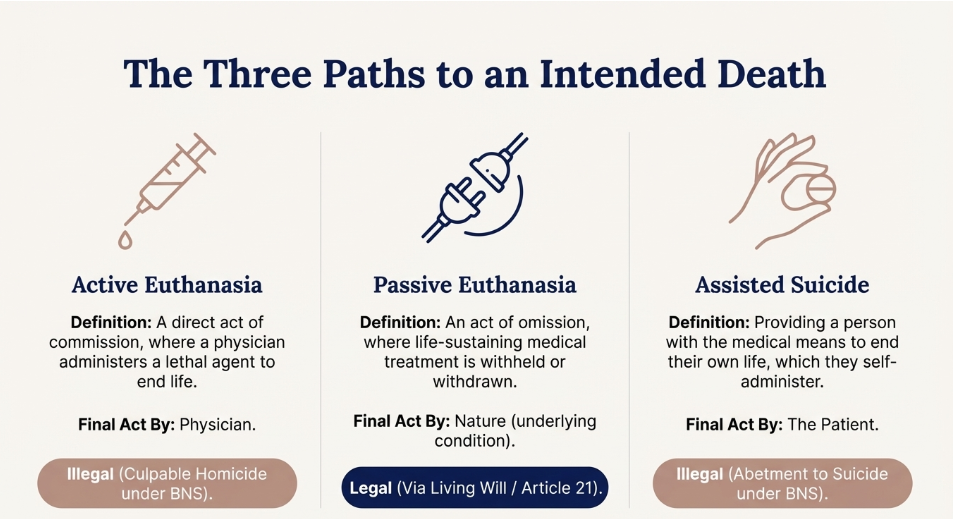
“Assisted Suicide is the clinical and ethical practice of intentionally providing a competent, terminally ill, or irremediably suffering individual with the medical means (such as a lethal prescription) or necessary information to terminate their own life, at their explicit and voluntary request, ensuring that the final, causal act of self-administration is performed by the patient.”
Active Euthanasia is defined by a direct intervention or an act of commission. In this scenario, a physician or third party introduces an external agent—most commonly a lethal injection of barbiturates—to deliberately and rapidly terminate the patient’s life. The primary intent is to end suffering through a swift, painless death. For example, in jurisdictions like the Netherlands, a doctor may administer a muscle relaxant followed by a drug to stop the heart of a terminally ill patient who has requested the procedure.
Passive Euthanasia, by contrast, is characterized by an act of omission or the withdrawal/withholding of life-prolonging measures. It occurs when medical professionals stop treatments that are merely “prolonging the act of dying” rather than curing the patient. Common examples include “Turning off a ventilator” (withdrawal) or “Not initiating chemotherapy” for a stage IV cancer patient (withholding). In these cases, the physician does not “kill” the patient; rather, they stop interfering with the inevitable biological end, allowing the patient to die of their underlying condition.
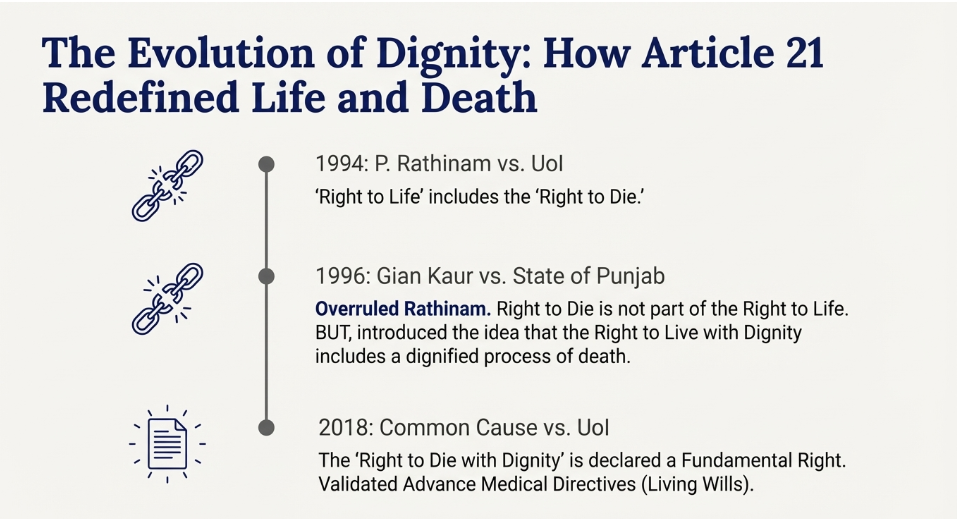
Article 21: “No person shall be deprived of his life or personal liberty except according to procedure established by law.”
Statutory Provisions & Bharatiya Nyaya Sanhita (BNS)
The criminalization of “ending a life” remains a cornerstone of Indian penal law, though the context of suicide has evolved.
Active Euthanasia: Under the BNS (2023), active euthanasia is not recognized as a separate category. It remains punishable as:
Attempt to Suicide (Section 226 of BNS): The BNS has significantly changed the old IPC Section 309. Attempting suicide is only a crime now if it is done with the intent to compel or restrain a public servant from performing their duty. This shift aligns with the Mental Healthcare Act (2017), which presumes that a person attempting suicide is under severe stress and requires rehabilitation, not punishment.
Abetment (Section 108 of BNS): Assisted suicide remains a grave offense. Providing the means for someone to end their life is treated as Abetment to Suicide.
A Living Will, formally known as an Advance Medical Directive (AMD), is a legal document that allows a person to state their medical treatment preferences in advance, specifically for a time when they may lose the capacity to make or communicate those decisions (e.g., irreversible coma or vegetative state).In India, the concept has evolved from being legally non-existent to a Fundamental Right under Article 21.
Because the 2018 guidelines were too “cumbersome” (requiring Judicial Magistrate approval), the SC modified them in January 2023 to make the process more practical:
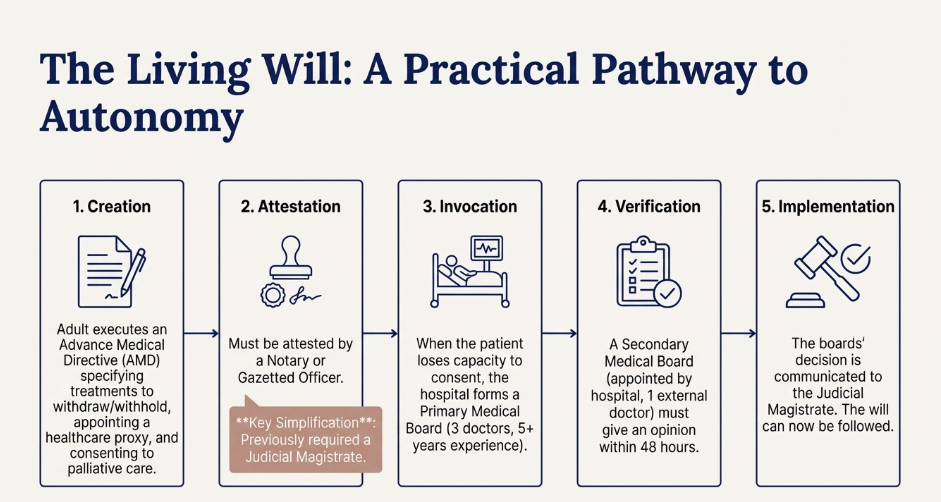
A valid Living Will in India typically includes three critical sections:
The Aruna Shanbaug vs. Union of India (2011) case is perhaps the most poignant and legally significant chapter in the history of Indian medical jurisprudence. It forced the Indian state to confront the “Right to Die” and created the first legal framework for passive euthanasia.
Aruna, who suffered irreversible brain damage from an assault, entered a Persistent Vegetative State (PVS), marked by “cortical blindness” and no cognitive awareness.
In 2009, journalist Pinki Virani, acting as Aruna’s “next friend,” petitioned the Supreme Court. She argued that Aruna’s existence was a “facade of life” and continuing Ryles tube feeding violated her right to a dignified life.
The Court rejected the plea to stop Aruna’s feeding, ruling she was not “brain dead” and that the KEM Nurses, not Pinki Virani, were her rightful “next friend.” As the nurses wished to keep her alive, the petition was dismissed. However, the case was used to legalize passive euthanasia in India, establishing judicial guidelines to be followed until Parliament passes a law.
The Supreme Court legalized Passive Euthanasia (omission) and deemed Active Euthanasia (commission) illegal, framing the Right to Die with Dignity as part of Article 21, provided the death is natural. The Court invoked the Parens Patriae Doctrine, mandating that the High Courts decide passive euthanasia pleas, not family, to prevent abuse. These petitions must be vetted by a Bench of at least two High Court judges based on a three-doctor committee report. This case paved the way for the Common Cause (2018) judgment on “Living Wills.”
Aruna Shanbaug eventually died of natural causes (pneumonia) on May 18, 2015, after 42 years in a vegetative state. Her case remains a symbol of the tension between medical technology’s ability to sustain “biological life” and the human need for “dignified death.”
Common Cause vs. Union of India (2018) case is the definitive legal authority that transformed passive euthanasia from a “judicially permitted exception” into a Fundamental Right.
In 2005, the NGO Common Cause filed a PIL arguing that modern medicine prolongs the suffering of the terminally ill, making the 2011 Aruna Shanbaug guidelines (which mandated impractical High Court intervention) insufficient. They sought to establish an individual’s autonomy for making advance decisions about life-prolonging treatment.
A 5-judge Constitution Bench led by CJI Dipak Misra addressed:
The Common Cause case has profoundly altered the landscape of medical ethics and law in India:
The Harish Rana vs. Union of India (2024-2025) case is the most significant contemporary legal battle regarding euthanasia in India. It represents the “final frontier” of the Right to Die with Dignity, challenging the medical and legal definitions of what constitutes “life support.”
In 2013, Panjab University student Harish Rana suffered a catastrophic Diffuse Axonal Injury from a fall, leading to 100% quadriplegia and a Permanent Vegetative State (PVS). He cannot move or speak, only breathing independently. By 2024, his aging parents, financially depleted from his care and unable to manage his severe bedsores and hopeless condition, petitioned the court for permission for euthanasia.
The case has moved through two critical judicial phases:
A. The Delhi High Court Phase (July 2024)
The High Court dismissed the parents’ plea.
The court cited the Common Cause (2018) ruling, which permits passive euthanasia only for those on “external/mechanical support.” As Harish was breathing independently and only required a “Ryles tube” (feeding pipe), the court deemed its removal “starving” him to death, classifying it as Active Euthanasia (illegal).
B. The Supreme Court Phase (Late 2024 – Jan 2025)
The parents appealed to the Supreme Court, whose Bench (Justices Pardiwala and Viswanathan) described Harish’s condition as “pathetic” and “very sad.”
The New Argument: Petitioners argue that “clinically assisted nutrition and hydration” (CANH) is a medical intervention, not just “food,” and withdrawing it should thus constitute Passive Euthanasia.
Current Status: As of late December 2025, the SC reviewed AIIMS reports confirming “negligible chances of recovery” and scheduled a personal meeting with the parents for January 13, 2026, for a “final call.”
The Harish Rana case is legally groundbreaking for three reasons:
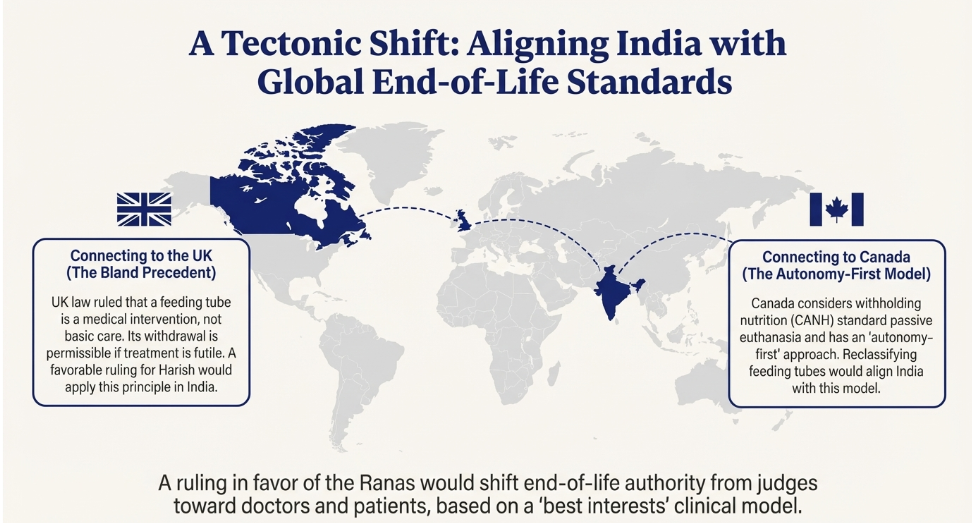
By revisiting the Harish Rana case in late 2025, the Supreme Court is essentially deciding whether to move India from a conservative “machine-dependent” model to a more modern “best-interests” medical model.
If the Supreme Court rules that feeding tubes (Clinically Assisted Nutrition and Hydration – CANH) are medical treatments, it would represent a “tectonic shift” in Indian law, bringing it in line with Western standards.
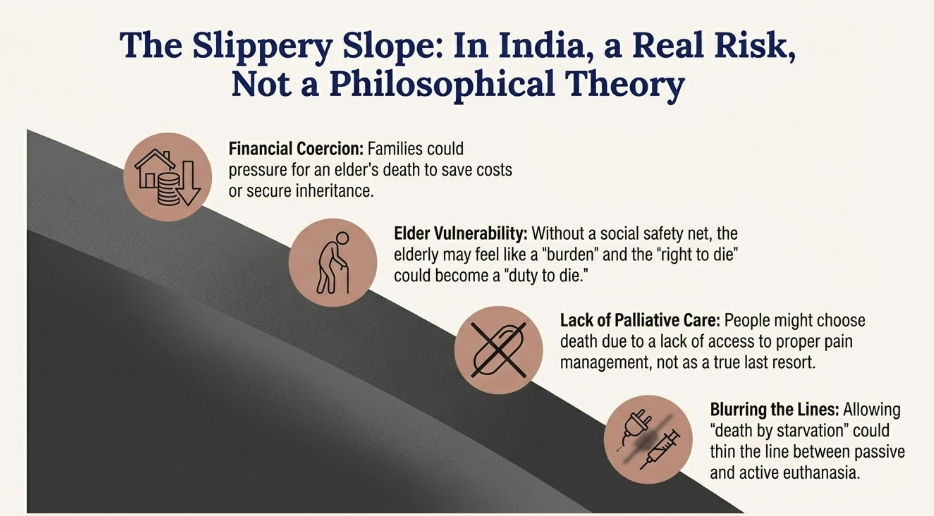
To prevent the “Slippery Slope” where the elderly might be coerced into a “duty to die,” we can brainstorm a multi-layered verification system that goes beyond simple medical boards.
Safeguards for Euthanasia and Withdrawal of Life Support
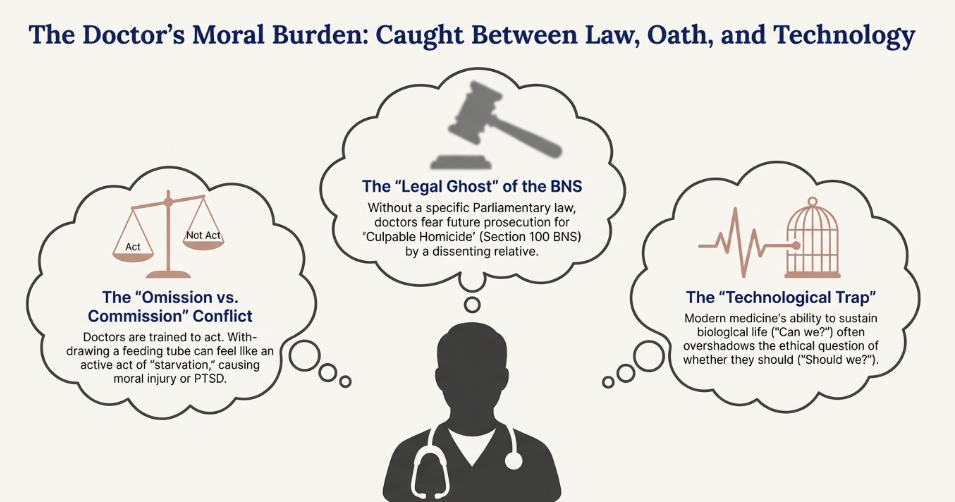
For a doctor, shifting from “Preserving Life” to “Withdrawing Sustenance” (the feeding tube) creates a profound Moral Injury.